Emergency Dialysis Catheter Insertion (IJV & Femoral)
Emergency Dialysis Catheter Insertion
Advanced Emergency Vascular Access Protocols Managed by Prof. (Dr.) Debabrata Mukherjee at Medanta – The Medicity, Gurugram.
Critical Access for Urgent Hemodialysis
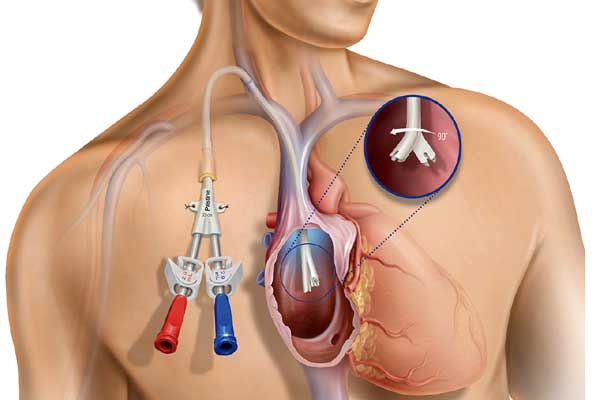
When acute toxin retention, severe metabolic acidosis, or life-threatening hyperkalemia occurs due to sudden renal shutdown, immediate blood purification is vital. Because a standard peripheral vein cannot support the high blood flow required for a hemodialysis machine, a specialized **Central Venous Catheter (CVC)** must be placed.
At Medanta Gurugram, clinical safety during this critical phase is our highest priority. **Prof. (Dr.) Debabrata Mukherjee** uses advanced, real-time ultrasound imaging to guide the placement of dual-lumen non-cuffed catheters, mapping structural anatomy precisely to maximize patient comfort and eliminate structural complications.
Clinical Mapping: Choosing the Optimal Access Route
| Clinical Metrics | Internal Jugular Vein (IJV Route) | Femoral Vein (Groin Route) |
|---|---|---|
| Anatomical Positioning | Lateral side of the neck (preferred primary site) | Groin area/Upper femoral triangle |
| Bacterial Contamination Risk | Significantly Lower | Higher (due to skin fold moisture) |
| Patient Mobility Index | Excellent (allows walking and sitting upright) | Restricted (strict bed rest to avoid kinking) |
| Safe Indwelling Lifespan | Temporary bridge up to 2–3 weeks | Emergency use only (limit to 3–5 days) |
1. The Ultrasound-Guided IJV Approach
The right internal jugular vein offers a direct, straight track into the superior vena cava, ensuring stable, high blood flows during dialysis cycles:
- Full surgical preparation under strict sterile barrier field conditions.
- Local subcutaneous anesthetic numbing block over the target tract.
- **Real-time ultrasound verification** of vein patency to prevent arterial crossover.
- Precise needle insertion via the **Seldinger wire technique**.
- Gentle tract dilation followed by placement of the flexible dual-lumen line.
- Suture anchoring and an immediate post-op portable chest X-ray check.
2. The Emergency Femoral Route
This route is selected when immediate access is required during extreme medical crises, or if acute neck anatomy issues prevent upper chest line placement:
- Rigorous sterilization of the upper femoral triangle and groin area.
- Targeted local sedation to ensure complete patient comfort.
- Vessel puncture executed safely below the inguinal ligament.
- Careful wire advanced to position the catheter within the inferior vena cava.
- Secure suturing and placement of an antimicrobial barrier dressing to prevent infection.
Advanced Safety & Risk Mitigation Protocols
Placing an central venous catheter requires meticulous care. Our clinical protocols at Medanta are designed to actively minimize procedural risks:
- Pneumothorax Prevention: Ultrasound guidance eliminates blind needle drops, reducing accidental lung-pleura nips to near zero.
- Arterial Protection: Visualizing the carotid or femoral artery under Doppler flow patterns prevents accidental arterial punctures.
- CRBSI Eradication: Utilizing specialized prophylactic antimicrobial locks and advanced chlorhexidine dressings to keep lines sterile.
- Thrombosis Mitigation: Using precise heparin flush ratios within the internal catheter lumens between dialysis runs to keep blood flowing smoothly.
Clinical FAQ: Dialysis Catheter Insights
Q1: How long can a temporary dialysis catheter remain in place safely?
Ans: A temporary non-cuffed Internal Jugular Vein (IJV) catheter can typically remain in place safely for 2 to 3 weeks under strict sterile management. Femoral catheters, due to their anatomical location in the groin, carry a much higher risk of bacterial contamination and are generally restricted to emergency settings, requiring removal or replacement within 3 to 5 days.
Q2: Can a patient shower or take a bath with a dialysis line?
Ans: No, a patient must absolutely never submerge or expose the dialysis catheter site to direct water. Moisture can easily disrupt the sterile dressing and allow skin bacteria to track down the line, resulting in a life-threatening Catheter-Related Bloodstream Infection (CRBSI). Sponge baths are recommended, keeping the catheter area fully dry.
Q3: What are the early signs of a dialysis catheter infection?
Ans: Early warning signs of a catheter-related infection include a high-grade fever, chills or shaking during dialysis cycles, localized redness, warmth, or oozing of pus at the insertion site. If any of these symptoms develop, immediate clinical evaluation by Prof. Dr. Mukherjee’s team is mandatory to determine if antimicrobial locks or line removal are required.
Prof (Dr) D Mukherjee is an alumnus of the prestigious Armed Forces Medical College, Pune where he did his MBBS & MD (Medicine). Subsequently he went on to do his DM (Nephrology) from PGIMER Chandigarh, which is the foremost training institution for nephrology in India.