Consent form for Hemodialysis
Consent form for Hemodialysis
Consent form for Hemodialysis
I,________________________________________ have been informed that my kidneys are not functioning and that I need hemodialysis to sustain my life. I understand that while hemodialysis is a life-sustaining procedure, it is not a cure for kidney failure.
The procedure necessary to treat my condition has been explained to me by my physician, and I understand the nature of the procedure to be as follows:
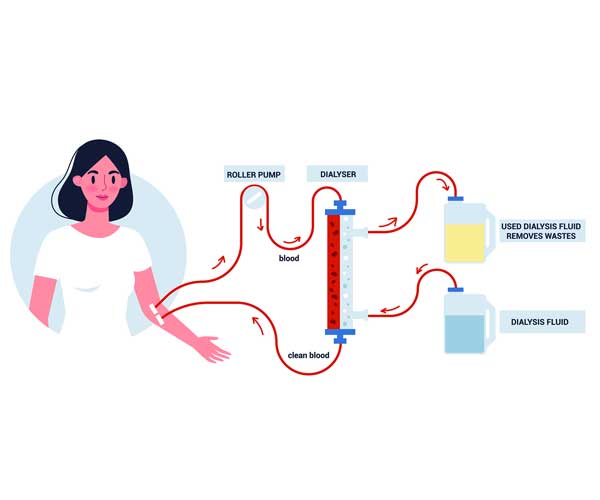
Hemodialysis will clean my blood by pumping it through a device that will remove wastes and excess fluids. I understand that hemodialysis involves, many things, the insertion of tubes and/or needles into my veins or fistula or through a catheter and the use of artificial kidneys to filter my blood. I also understand that, along with the hemodialysis treatment, I may need laboratory tests, radiology, and surgical procedures to assure the adequate function of the equipment and the effectiveness of the treatment. In addition, the use of blood thinners such as heparin is required to provide effective dialysis and prevent the clotting of the blood.
I have been informed that the following risks are associated with hemodialysis and that while such risks are not common, one or more can occur and be potentially life-threatening:
- Bacterial and/or viral (e.g., Hepatitis B or C) contamination of my blood which may cause infection or bacterial infection of the blood called Sepsis;
- Bleeding due to blood clotting problems or disconnection of blood tubing;
- “Destruction” or the breakdown of red blood cells, known as hemolysis;
- Internal bleeding or bleeding from the access site;
- Infections of my access site (catheter or fistula infections);
- Introduction of air into my bloodstream;
- Shock or cardiac arrest;
- Allergic and toxic reactions to drugs, solutions, artificial kidneys, or other equipment used during the hemodialysis treatment.
- Clotting of my access or infiltration of my access.
I have also been informed that there may be some side effects associated with hemodialysis related to fluid and chemical changes during or after the hemodialysis treatment. Some of the side effects are osteoporosis, electrolyte imbalance, headache, nausea, dizziness, fainting, irregular heartbeats, decrease in blood pressure, muscle cramping, and mild confusion.
The hemodialysis procedure and the alternatives to hemodialysis have been explained to me.
I understand the alternatives to hemodialysis to be: peritoneal dialysis, or transplantation, and that I may be evaluated for either whenever I choose.
I understand that it will be necessary for me to follow certain dietary restrictions. It will be my responsibility to follow these dietary restrictions and failure to do so can cause bone disease, calcification of my heart, blood vessels and skin, heart failure, and even sudden death. In addition, I understand that it will be my responsibility to take my medication as prescribed by my physician. The success of hemodialysis also depends upon my agreeing to remain on the machine for the prescribed length of time so that my blood can be adequately cleansed.
I will immediately notify my physician of any adverse reactions or problems I may have with regard to these hemodialysis treatments.
I authorize repeated hemodialysis treatments unless I specifically revoke this consent. This consent will be renewed on or about an annual basis.
I have read this consent and fully understand its contents. I have had a chance to have my questions answered in words I can understand. I hereby execute this consent form freely and with full acceptance and knowledge of the contents in it. I also understand that this is a legal document.
__________________________________Date _______Time:__________
Patient or Legally Authorized Representative
__________________________________Date _______Time:__________
Physician Signature
__________________________________Date _______Time:__________
Witness Signature