Consent For Insertion of Dialysis Catheter
CONSENT FOR INSERTION OF DIALYSIS CATHETER
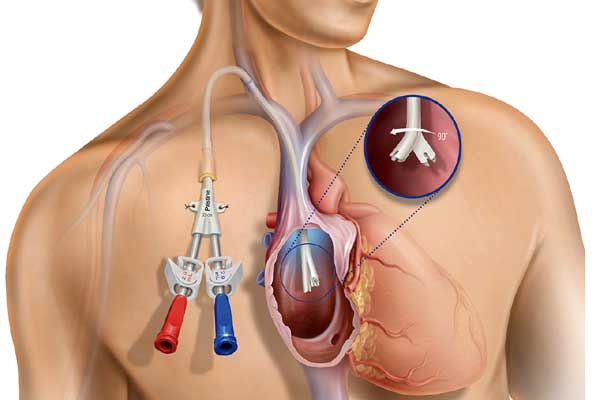
I have been explained that I need vascular access to provide hemodialysis. As I dont have an AV Fistula I need a temporary double lumen/ triple lumen catheter or a tunnelled cuffed dialysis catheter to initiate dialysis. The catheter will be placed in the internal jugular/ femoral vein. This procedure will require an injection of local anaesthetic and a sedation anaesthetic.
In recommending the study, the doctor believes the benefits to you from having this procedure exceed the risks involved. The risks and complications with this procedure can include but are not limited to the following.
Common risks and complications include:
- Minor pain, bruising and/or infection from the IV cannula. This may require treatment with antibiotics
- Pain or discomfort at the insertion site. This may require medication
- Bleeding or bruising may occur. This is usually stopped by applying further pressure and/or ice to the puncture site. This is more common if you -take Aspirin, Warfarin, Clopidogrel or Dipyridamole
- The device may become kinked/ blocked requiring removal/ repositioning or medications for unblocking
- Tunnelled and Non-tunnelled catheters only) The catheter may be accidentally removed if pulled or tugged on.
- Failure of local anaesthetic which may require a further injection of anaesthetic or a different method of anaesthesia may be used.
- Nerve damage, is usually temporary, and should get better over a period of time. Permanent nerve damage is rare.
Less common risks and complications include:
- Infection at the skin, requiring antibiotics and/or further treatment.
- Infection in the device, requiring the device to be removed.
- Pneumothorax, a collection of air around the lining of the lungs. This usually resolves by itself but sometimes may require a tube to be inserted into the chest.
- Damage to surrounding structures such as blood vessels, organs and muscles, requiring further treatment.
- Failure to gain access to the vein. This may require a second attempt from a different location.
- Blood clot blocking the vein, may require medication to treat.
- An allergy to injected drugs, requiring further treatment.
- The procedure may not be possible due to medical and/or technical reasons.
Rare risks and complications include:
- Injected medications may leak outside of the vein under the skin and into tissue, this may require treatment.
- A fast or irregular heart beat. This usually resolves on it’s own but sometimes may need further treatment.
- The catheter tip may move from the original placement. The device may need to be removed.
- An air bubble enters the blood stream. This can travel to the heart causing a heart attack or to the brain causing a stroke.
- An increased lifetime cancer risk due to the exposure to x-rays.
- Seizures and/or cardiac arrest due to local anaesthetic toxicity.
- Death as a result of this procedure is very rare.
Patient Consent
I acknowledge that the doctor/doctor delegate has explained the proposed procedure.
I understand;
- The risks and complications, including the risks that are specific to me.
- The sedation/anaesthetic required for this procedure. I understand the risks, including the risks that are specific to me.
- That no guarantee has been made that the procedure will improve my condition even though it has been carried out with due professional care.
- If immediate life-threatening events happen during the procedure, they will be treated based on my discussions with the doctor/doctor delegate or my Acute Resuscitation Plan.
- A doctor/doctor delegate undergoing further training may conduct this procedure.
- I was able to ask questions and raise concerns with the doctor/doctor delegate about the proposed procedure and its risks. My questions and concerns have been discussed and answered to my satisfaction
- I understand I have the right to change my mind at any time including after I have signed this form but, preferably following a discussion with my doctor/doctor delegate
- I understand that image/s or video footage may be recorded as part of and during my procedure and that these image/s or video/s will assist the doctor to provide appropriate treatment
- I understand that Medanta Medicity Hospital may release my relevant de-identified information obtained from this and related procedures for education and training of health professionals
On the basis of the above statements,
I request to have the procedure
Name of Patient:…………………………………………………………………………………………………………..
Signature: ……………………………………………………………………………………………………………….
Date:…………………………………………………………………………………………………………………….