Dialysis for Kidney Failures
Prof. (Dr.) Debabrata Mukherjee | Advanced Dialysis & Renal Replacement
Senior Director – Nephrology & Renal Transplant, Medanta – The Medicity, Gurugram
Renal Replacement Therapy: Optimizing Life-Sustaining Clearance
When chronic kidney damage advances to **End-Stage Renal Disease (ESRD)**, or when an acute injury precipitates sudden organ shutdown, the body loses its core ability to filter metabolic waste products, balance blood minerals, and excrete fluid. Without intervention, toxic compounds quickly accumulate, leading to severe clinical complications like **Uremic Syndrome** or fluid overload in the lungs.
At our dedicated facility inside **Medanta Sector 38, Gurugram**, we provide highly advanced **High-Flux Hemodialysis** alongside tailored **Peritoneal Dialysis** regimens. Supervised closely by **Prof. (Dr.) Debabrata Mukherjee**, our dialysis protocols focus on achieving exceptional uremic clearance, maintaining cardiovascular stability, and serving as a safe, healthy bridge to a kidney transplant for patients across Gurugram and the wider Delhi-NCR region.
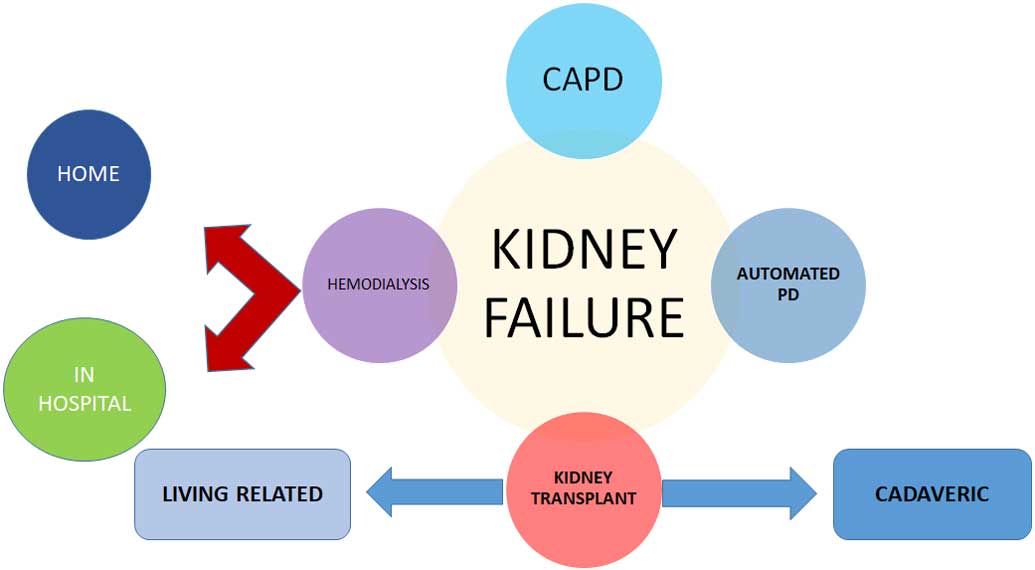
Primary Dialysis Modalities
1. Clinical Hemodialysis (HD)
Extracorporeal filtration where blood is pumped through an advanced synthetic dialyzer (artificial kidney). Done under continuous nursing and nephrology observation, this modality generally requires three scheduled outpatient sessions per week at our fully equipped Gurugram hub.
2. Peritoneal Dialysis (PD)
An internal, home-based therapeutic option where sterile dialysate solution is instilled directly into the abdominal cavity. The patient’s native peritoneal membrane serves as the filter, utilizing gravity-fed or automated cycler exchanges to remove toxins seamlessly overnight or throughout the day.
Clinical Indicators for Dialysis Initiation
Therapy is initiated when a patient displays systemic signs of advanced kidney failure:
- Uremic Pericarditis or Uremic Encephalopathy (cognitive slowdown or confusion).
- Refractory Hyperkalemia (critically high potassium levels non-responsive to medications).
- Severe fluid overload or fluid in the lungs triggering acute shortness of breath.
- Persistent, unmanageable nausea, severe metabolic acidosis, or profound muscle wasting.
Primary Systemic Causes
Progressive loss of kidney structure leading to dialysis dependency is typically driven by:
- Diabetic Nephropathy (advanced microvascular kidney damage from long-standing diabetes).
- Malignant Nephrosclerosis (uncontrolled systemic high blood pressure).
- Chronic Glomerulonephritis (immune-mediated structural destruction of glomeruli).
- Rapidly progressing Autosomal Dominant Polycystic Kidney Disease (ADPKD).
Advanced High-Flux Dialysis Infrastructure
Traditional low-flux therapy relies almost entirely on passive diffusion to remove basic small molecules like urea. In contrast, our unit utilizes premium **High-Flux Hemodialysis membranes**, which offer significant clinical improvements:
Larger pore sizes facilitate convective transport, efficiently removing larger uremic toxins such as Beta-2 Microglobulin ($β_2-M$).
Minimizes dialysis-induced vascular stress and hemodynamic drops, protecting cardiac tissue and reducing long-term calcification risks.
By clearing advanced glycation end-products, it lowers systemic inflammatory scores, improving overall vitality and nutrition levels.
The Nephrologist’s Management Framework
A successful dialysis outcome requires continuous, highly personalized medical adjustments. **Prof. (Dr.) Debabrata Mukherjee** customizes every aspect of care—including determining optimal blood pump flow speeds ($Q_b$), selecting dialysate composition profiles, managing dry weight metrics, and ensuring precise anemia and bone-mineral stabilization. Additionally, our medical team focuses on the careful preservation of vascular health (such as managing **AV Fistulas** or **PermCaths**) to maintain high-quality, long-term therapeutic access.
Clinical FAQ: Navigating Dialysis Therapy
Q1: What is the clinical advantage of High-Flux Hemodialysis over conventional Low-Flux Dialysis?
Ans: High-Flux Hemodialysis utilizes highly permeable synthetic membranes with larger pore sizes. This allows for both diffusive and convective mass transport, effectively clearing middle-sized uremic molecules like Beta-2 Microglobulin ($β_2-M$). Removing these larger toxins significantly reduces chronic inflammation, lowers amyloidosis risks, and provides superior long-term cardiovascular protection compared to standard low-flux units.
Q2: How is vascular access monitored and preserved between dialysis sessions?
Ans: Vascular access—whether an AV Fistula, AV Graft, or tunneled PermCath—requires strict infection control and flow monitoring. Patients must check for a continuous physical vibration (‘thrill’) and a rhythmic sound (‘bruit’) daily over their fistula site. To prevent access thrombosis or clotting, drops in blood pressure, heavy compression on the access arm, and tight clothing must be strictly avoided.
Q3: Can a patient remain on high-flux dialysis indefinitely, or is it strictly a bridge to a transplant?
Ans: High-flux dialysis can safely serve as a long-term maintenance therapy for patients who are not candidates for renal transplantation due to extensive comorbidities. However, for eligible individuals, our unit structures the dialysis protocol to optimize physiological health, maintain cardiovascular parameters, and serve as an ideal bridge to a kidney transplant.