Polycystic Kidney Disease (PKD) Treatment
Understanding Polycystic Kidney Disease (PKD)
Discovering that you or a family member has Polycystic Kidney Disease (PKD) can be overwhelming. Because it is a genetic condition passed down through generations, families often carry a deep-seated fear of kidney failure. PKD causes multiple fluid-filled cysts to grow inside the kidneys, making them enlarge over time and impacting their ability to filter waste.
However, a diagnosis does not mean immediate kidney failure. With recent medical breakthroughs, we can significantly slow down the growth of these cysts. Prof. (Dr.) Debabrata Mukherjee offers a compassionate, international standard of care ranging from early genetic mapping to advanced targeted therapies.
+91 8130060240
The Two Sides of PKD: Types & Genetics
PKD is primarily categorized into two distinct types based on how the faulty gene is inherited from parents:
1. Autosomal Dominant PKD (ADPKD) — The Adult Form
This is the most widespread variant, accounting for nearly 90% of all PKD cases. If just one parent carries the mutated gene (either PKD1 or PKD2), there is a 50% chance of passing it to the child.
- When it appears: Cysts develop silently for years; symptoms typically show up between ages 30 and 50.
- Gene Impact: Mutations in the PKD1 gene generally progress slightly faster than mutations in the PKD2 gene.
2. Autosomal Recessive PKD (ARPKD) — The Infantile Form
This is a much rarer and more severe form that manifests early in life. For a child to develop ARPKD, both parents must carry a copy of the mutated PKHD1 gene.
- When it appears: It is usually diagnosed during routine pregnancy ultrasounds or right after birth.
- Key Signs: Infants often display breathing difficulties due to underdeveloped lungs, along with severe liver issues.
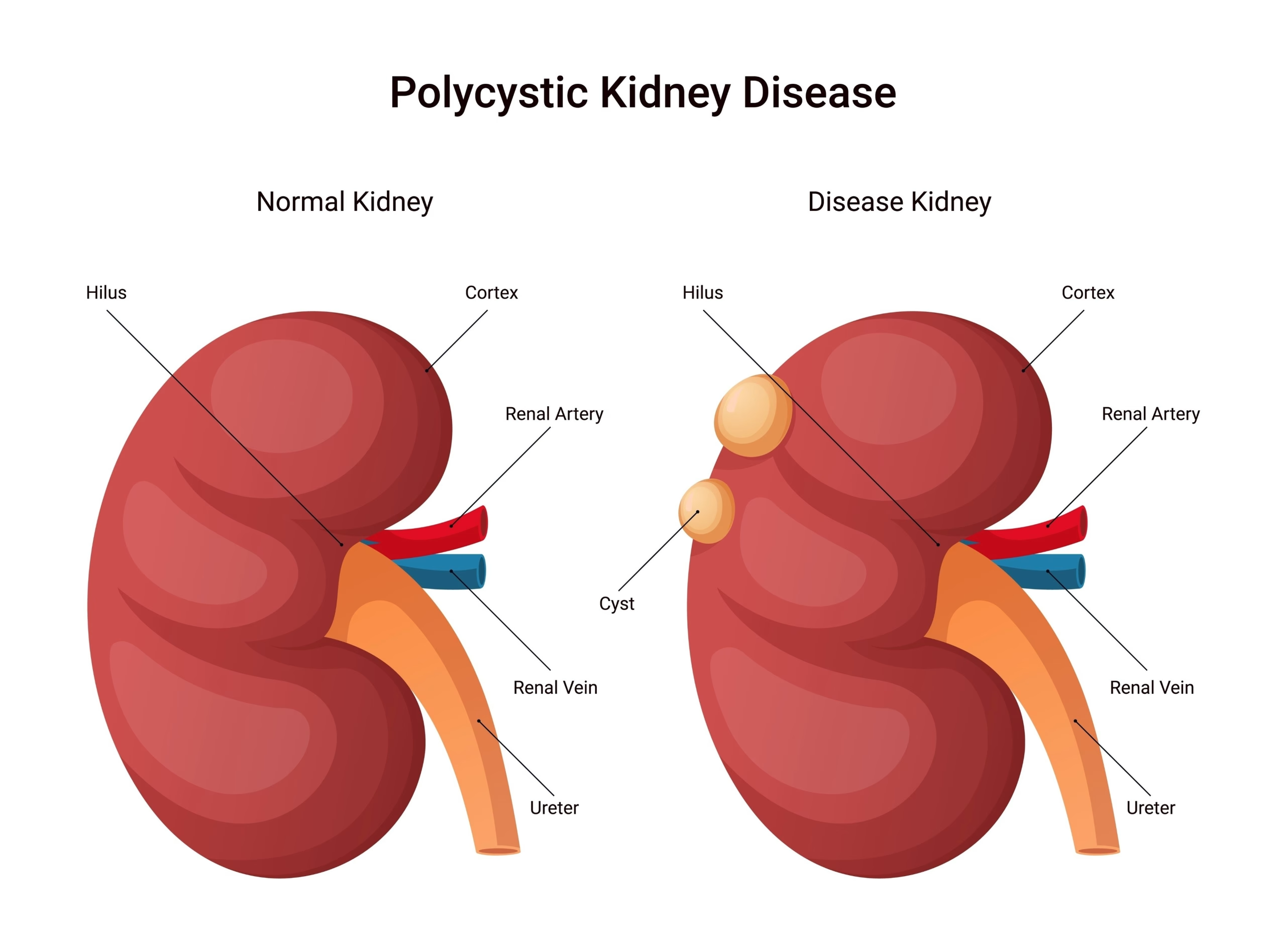
Understanding the Anatomy of PKD
Polycystic Kidney Disease (PKD) is characterized by the growth of numerous fluid-filled cysts within the kidneys. Unlike a healthy kidney, which maintains a smooth, bean-shaped structure, a polycystic kidney can enlarge significantly over time.
As seen in the visual, the accumulation of these cysts disrupts the normal filtering architecture of the nephrons. Early intervention and imaging are crucial to monitor these structural changes and preserve renal function.
Symptoms: When Should You See a Specialist?
In its early stages, PKD behaves like a silent condition. However, as fluid inside the cysts expands, the increasing size of the kidneys triggers clear physical distress signals:
ADPKD (Adult) Symptoms
- Chronic dull ache in the lower back or sides (flanks)
- Unexplained, stubborn high blood pressure
- Visible blood in urine (Hematuria) from bursting cysts
- Recurrent kidney stones and painful UTIs
- A feeling of fullness or swelling in the abdomen
ARPKD (Child) Symptoms
- Massively enlarged kidneys noticeable at birth
- Severe respiratory distress or lung underdevelopment
- Early-onset liver scarring (hepatic fibrosis)
- History of low amniotic fluid levels during pregnancy
Precision Diagnosis
Treating PKD effectively depends on predicting how fast it is growing. Prof. (Dr.) Mukherjee uses advanced imaging technologies to measure Total Kidney Volume (TKV), which acts as a crucial roadmap to determine how aggressively we need to treat the condition.
- High-Resolution Ultrasound: The standard, radiation-free method used to spot and count cysts in families with a history of PKD.
- Advanced MRI/CT Scans: Essential for mapping accurate TKV scores to track disease progression over time.
- Targeted Genetic Testing: Specialized blood tests to detect precise mutations within the PKD1, PKD2, or PKHD1 genes—highly recommended for family planning.
Modern Treatment & Management Protocols
While there is no permanent genetic cure to reverse PKD yet, modern nephrology allows us to manage symptoms expertly and safeguard your long-term health:
1. Disease-Modifying Therapy (Tolvaptan Protocol)
This is a major medical milestone in treating adult ADPKD. Tolvaptan is a targeted drug that blocks the activity of vasopressin—a hormone that feeds fluid into the cysts. When started at the right stage under Prof. (Dr.) Mukherjee’s precise supervision, it slows down cyst expansion, effectively delaying the need for dialysis by years.
2. Strict Cardiovascular Protection
High blood pressure accelerates kidney damage in PKD. We utilize specialized ACE inhibitors or ARBs that protect the heart while easing the structural stress placed on your kidneys. This is supported by low-sodium dietary tracking and high fluid intake protocols to lower cyst-stimulating hormones.
3. Advanced Care for End-Stage Renal Disease (ESRD)
If the disease progresses to advanced stage renal failure, Prof. (Dr.) Mukherjee provides seamless transitions into world-class maintenance Dialysis or Pre-emptive Kidney Transplantation. Our high-volume transplant experience ensures excellent long-term graft survival rates for patients with enlarged genetic kidneys.
Frequently Asked Questions (FAQs)
Q1: Does having a parent with PKD mean I will definitely inherit it?
If a parent has Autosomal Dominant PKD (ADPKD), there is a 50% chance of passing the gene down to each child. If you inherit the gene, you will develop cysts, but the severity and speed of progression vary from person to person. Genetic counseling can provide clearer answers.
Q2: Is Tolvaptan therapy suitable for every PKD patient?
No. Tolvaptan is specifically prescribed for adult ADPKD patients who show signs of rapidly progressing disease. It requires regular monthly blood tests to monitor liver health, which is why it is managed under strict clinical guidelines.
Q3: Do the cysts spread to other parts of the body outside the kidneys?
Yes, it is possible. Over time, individuals with PKD may develop benign cysts in the liver or pancreas. While liver cysts rarely cause organ failure, they can cause abdominal fullness, which we manage with lifestyle and targeted clinical adjustments.
Protect Your Family’s Health
Early diagnostic screening and modern therapies can delay the progression of genetic kidney cysts.
Personal Assistant:
Direct Desk Email:
dirnephro@gmail.com
Location:
Gurugram, India
Medically Reviewed & Approved By:

Prof. (Dr.) Debabrata Mukherjee
Senior Director & Senior Consultant – Nephrology & Renal Transplant,
Medanta – The Medicity, Gurugram.
With a focus on managing progressive PKD and polycystic kidney complications, he provides evidence-based, compassionate care for the most challenging clinical cases.