Peritoneal Dialysis Catheter Insertion
Prof. (Dr.) Debabrata Mukherjee | Home Dialysis Surgery
Senior Director – Nephrology & Renal Transplant, Medanta – The Medicity, Gurugram
Peritoneal Dialysis Access: Empowering Patients at Home
**Peritoneal Dialysis (PD)** offers an advanced, highly flexible home-based alternative to traditional hemodialysis. Instead of an external machine membrane, this method utilizes the patient’s own **peritoneal membrane** inside the abdomen to filter out metabolic wastes, excess toxins, and retained fluids continuously.
To facilitate this, a specialized, highly flexible **Tenckhoff Catheter** must be surgically placed into the lower abdominal cavity. Under the medical direction of **Prof. (Dr.) Debabrata Mukherjee at Medanta Sector 38**, PD catheter insertion is completed using advanced open or laparoscopic techniques, ensuring optimal fluid flow mechanics and a seamless transition to home-based renal care for patients throughout Gurugram and Delhi-NCR.
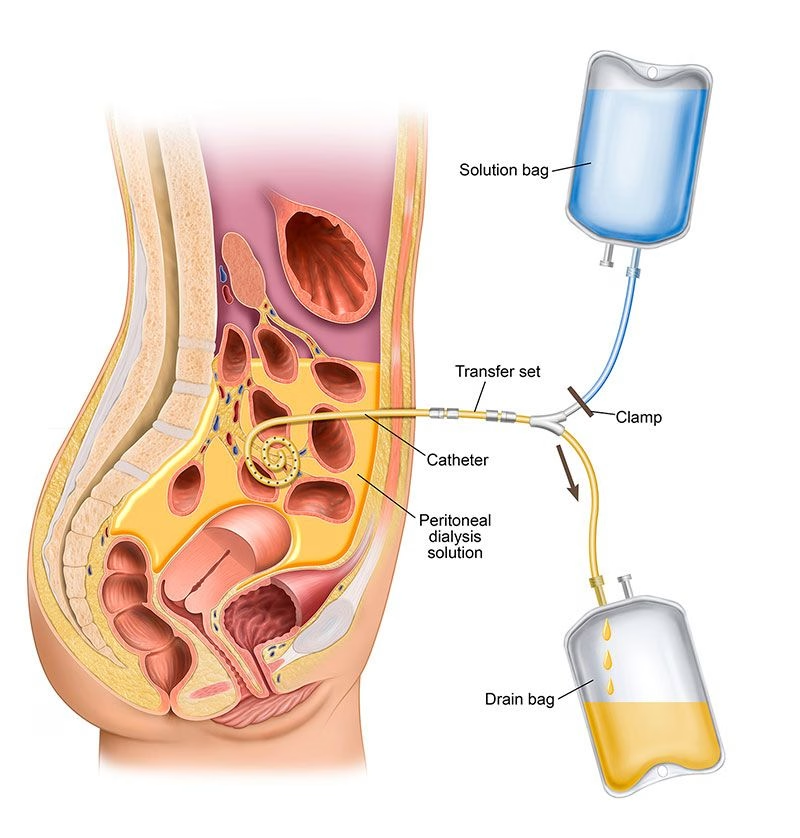
Standard Peritoneal Dialysis Flow System
Surgical Placement Overview
The biocompatible silicone Tenckhoff line is placed into the deepest portion of the pelvic peritoneal recess. This precise placement ensures maximum fluid drainage and prevents long-term line migration or catheter displacement during daily fluid exchanges.
Preoperative Optimization
- Careful mapping of the abdominal wall to select an exit site clear of scars or skin folds.
- Comprehensive ruling out of active abdominal hernias or complex intra-abdominal adhesions.
- Administration of targeted prophylactic antibiotic drops to minimize surgical site contamination.
Surgical Standard: Executing Catheter Placement
- Sterile Operational Setup: Conducted inside Medanta’s modular operating suites under local anesthesia with sedation or general anesthesia.
- Primary Abdominal Incision: A small incision is mapped out, piercing carefully through the anterior rectus sheath.
- Pelvic Recess Placement: The multi-hole segment of the Tenckhoff line is guided deep into the true pelvis to capture fluid easily.
- Double-Cuff Anchoring: Internal and external Dacron cuffs are positioned securely to seal the pathway and lock out ascending pathogens.
- Subcutaneous Tunneling: The outer section of the line is tunneled sideways beneath the skin, terminating at a clean, downwards-pointing exit-site.
Post-Operative Healing & Care
- Daily inspection of the exit-site for any early tracking, clear fluid oozing, or skin breakdown.
- Enforcing strict dry-dressing techniques using premium sterile materials.
- Restricting abdominal muscle strain and heavy lifting for at least 2 to 3 weeks post-surgery.
- The 14-Day Rule: Allowing a full 2-week tissue integration window before starting full-volume dialysate flushes.
Complication Mitigation Protocols
We closely monitor patients to prevent, identify, and manage any advanced access risks:
- Peritonitis: Managed instantly using specialized intraperitoneal antimicrobial regimens.
- Outflow Failure: Cleared via postural movement, targeted laxatives, or low-dose fibrinolytic locks.
- Abdominal Wall Hernia: Prevented by calculating dialysate volume parameters based on core structural support.
Why Clinical Teams Select Peritoneal Access
Home Autonomy
Allows therapy to be managed conveniently during overnight sleep cycles or regular daytime routines.
Hemodynamic Stability
Gentle, continuous waste removal mimics natural renal kinetics, avoiding rapid drops in blood pressure.
Preserved Residual Function
Sustains remaining baseline kidney filtration capacities for a longer duration compared to hemodialysis.
Clinical FAQ: Navigating Peritoneal Dialysis Access
Q1: How soon can a patient start peritoneal dialysis after the catheter insertion surgery?
Ans: Typically, a healing period of 2 weeks (14 days) is highly recommended before standard high-volume dialysate exchanges begin. This prevents fluid leaks around the incision lines. However, in urgent situations, low-volume supine (lying down) dialysis can be initiated earlier under strict clinical supervision in our Medanta unit.
Q2: What are the primary symptoms of peritonitis, and how is it treated?
Ans: The primary signs of peritonitis include cloudy effluent (dialysis fluid draining out), sudden severe abdominal pain, fever, nausea, or redness around the catheter exit-site. Peritonitis is a medical emergency and is aggressively managed by Prof. Dr. Mukherjee using intraperitoneal antibiotics added directly into the dialysis solution.
Q3: What causes inflow or outflow failure in a PD catheter, and how is it fixed?
Ans: Inflow or outflow blockages are generally caused by internal catheter migration, kinking, blood clots, or fibrin webs blocking the line tips. Clinical solutions include using internal heparin flushes, treating constipation (which alters bowel pressure against the line), or repositioning the catheter tip using low-dose fluoroscopic guidance.